

As a hypermobility coach, I often encounter patients who have been misdiagnosed or undiagnosed with hypermobility disorders due to the limitations of the Beighton score. While the Beighton score is a useful tool for assessing joint hypermobility, it is not the end-all-be-all for diagnosing hypermobility disorders such as hEDS/HSD. In fact, relying solely on the Beighton score can lead to many patients being misdiagnosed or undiagnosed.
What is the Beighton score?
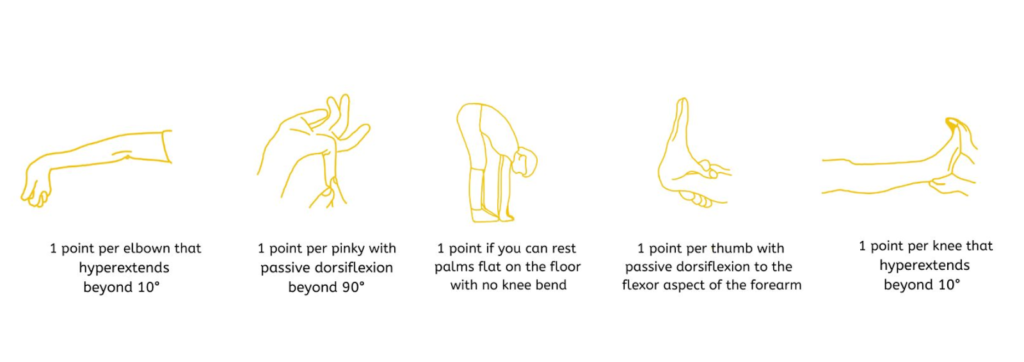
The Beighton score is a tool used to assess joint hypermobility, which is currently the only score used in the hEDS diagnostic checklist. It consists of a series of movements that assess the range of motion in the joints, and a score out of 9 possible points is given based on the number of movements that can be performed. The score cutoffs vary depending on age and gender, with different cutoffs for children, adolescents, and adults.
Beighton score:
≥6 pre-pubertal children and adolescents
≥5 pubertal men and woman to age 50
≥4 men and women over the age of 50
The benefits and strengths of the Beighton score:
One of the strengths of the Beighton score is its ease of use – it is performed quickly and easily without needing any equipment. It also has great inter- and intra-reliability, meaning that if one doctor says a patient “passes,” it is very likely that other doctors will agree.
What doesn’t the Beighton score account for?
However, it has some limitations as well. The Beighton score does not account for pain, function, or other symptoms, and its ability to truly reflect generalized joint hypermobility has been questioned. Additionally, the Beighton score has extremely wide ranges of specificity and sensitivity, and no studies have been done to test its validity from a diagnostic standpoint. This means that relying solely on the Beighton score for diagnosis can result in a significant number of missed diagnoses.
The limitations of the Beighton score:
One of the main limitations of the Beighton score is that it primarily focuses on the upper extremities, which may not accurately reflect generalized joint hypermobility. Additionally, the Beighton score does not account for pain, function, or other symptoms that may be present in patients with hypermobility disorders. This can result in patients being misdiagnosed or undiagnosed despite presenting with symptoms of hEDS/HSD.
Other helpful scoring systems and diagnostic tools:
It is important for both patients and clinicians to understand the limitations of the Beighton score and to seek out additional assessments if hEDS/HSD is suspected. Other scoring systems and diagnostic tools are available and should be used if you suspect a patient is struggling with hEDS/HSD and they do not “pass” the Beighton score. The other scales that can be used include
- The 9-point Beighton modification
- The Hospital del Mar criteria
- The Rotes-Querol scale
- 5pq
- The Carter-Wilkinson criteria
- The Windsor scale
If you suspect that you may have hEDS/HSD or if you have been misdiagnosed or undiagnosed due to the limitations of the Beighton score, I encourage you to seek out a specialist in your area. The Ehlers Danlos Society Providers List is a great resource for finding specialists who can accurately diagnose and treat hypermobility disorders.
Seeking hypermobility support?
If you have any questions or concerns about hypermobility disorders, I would love to connect with you on a discovery call where we will discuss your individual situation and decide together how I can support you during your hypermobility journey.
If you’re struggling with hypermobility disorders, I understand how overwhelming it can be, read about my story here. I’m here to support you every step of the way!
Reference:
Hurst, B., Krahn, J., Harmsen, S., et al. (2022). Beighton score alone fails to diagnose the majority of patients with hypermobile Ehlers-Danlos syndrome: A retrospective analysis of a multicenter EDS cohort. medRxiv. doi: 10.1101/2022.04.25.22274226.